

Rare Disease Is a Health Inequality: It’s Time for UK Policy to Reflect That
I’ve been levelling up
I have been a Commissioner on the Lancet Commission for Rare Disease for two years and we are fast approaching the point of writing up our findings and recommendations. I have been working alongside a team of other Commissioners, who bring a vast wealth of knowledge and experience in different areas, from different parts of the globe.
I have developed a new foundation of understanding in Human Rights, thanks to the patience of Professor Bartha Knoppers. I’ve had the opportunity to share thoughts with the incredible Dr Ana Rath from Orphanet (who now keeps me up-to-date on the official number of rare diseases identified via WhatsApp… 6659 at time of writing!) I have been working on a modified Delphi study with a team from the Children’s Hospital of Eastern Ontario, headed up by Dr Kim Boycott. And just to remind me of what a small world we live in, one of my Commissioner buddies, Kirsten Johnson (Chair of Rare Diseases International) lives only 16 minutes away from me… a fact was not given away by her accent, which I hope she won’t mind me calling ‘eclectic!
Social justice and rare disease
In this time I have been examining social justice for the Rare Disease Community. We’re all born equal in dignity and rights, and yet that just doesn’t ring true when you look back at the decades of reports on rare lived-experience. I grew up in a household where I observed in real time the advent of new technology that could sequence my deceased brother’s DNA. I collected data for natural history studies and met people who flew across the globe to take part in clinical trials for the first ever specific therapy for his condition. I celebrated at the end of the clinical trial party and watched a man, I had grown up with, take the first steps in years, following treatment. I have deep appreciation of the incredible efforts of individuals across sectors that have led to the advancement of the Rare Community today.
The progress in advocacy, medicine and technology were once unfathomable. However what I struggle with is the fact that the benefits of these advances are often inaccessible, inequitable or applied on the background of severe deprivation. Someone may have the most outstanding and informed care 200 miles away from home in their specialist centre but be fearful to visit their local hospital in times of need. Or they may be unable to access care for regular health concerns due to their GP’s fear of not being familiar with their underlying rare condition. According to the Rare Barometer survey by EURORDIS, people with rare conditions are those most likely to miss out on school and be discriminated against in society, due to their disability. This disparity between highly specialised care and basic social and health care in one nation can sometimes have me tearing hair out. It all just feels so…unfair! Being part of the Lancet Commission has helped me to understand that this feeling comes from the very real injustice facing the rare community. Hopefully, over time, I will also become more eloquent at communicating it as well… here is my first attempt.
Rethinking Rare Disease in the UK
I am reflecting on how I can bring my learnings from the Commission work back to the UK, where Medics for Rare Disease is based. As the Commission will show, any country thinking it is looking after the rare community well is deluded. As for countries who claim they are ‘pioneers’ in Rare Disease – well, we all know the impact of British pioneers on the people they were supposedly helping and it’s not something I would like to claim the title of. I feel like I have a fresh perspective now that I am looking at the challenges through the lens of Human Rights legislature: the Right to Health, the Right to non-discrimination, the Right to Self-Determination, the Right to Education, the Rights of the Child and the Right to Science. Having looked at the evidence it is hard to come to any other conclusion than the sad reality that the UK is not equitably delivering on these rights. This is despite over 10 years of policy and huge investment in certain areas. I think it’s time to flip the script. Instead of “How can the UK not be the best at the development of technologies and therapies”, could the UK aspire to be “the best at delivery of holistic healthcare to the rare community”?
These are, after all, the patients that made such technologies and therapies possible. We need a different way to approach Rare Disease policy. Fortunately the United Nations and World Health Organisation are leading the way.
Rare Disease causes health inequalities
The Rare Disease Community is a defined population that, as a group, are disadvantaged in society and healthcare. Like other marginalised groups they experience avoidable and discriminatory health inequalities because the systems that serve them are not accessible to them or designed for their unique but collective needs.
The core challenge for people living with rare disease in the NHS is that they’re disadvantaged through health inequalities. Once we acknowledge this fact we can start unpicking the root causes of the inequalities. We can also start applying already available frameworks (such as Core20PLUS5), systems and laws to ensure this group is protected and their health is promoted. It will also move this conversation away from “golden bullet” solutions – which are usually a health science innovation such as advanced testing and therapies or AI. We can re-centre the conversation to the lived experiences of the people living with rare diseases and those and caring for them.
What if we don’t address Rare Disease as a Health Inequality?
Even if we don’t acknowledge the role of discrimination and health inequalities in the rare disease experience, it doesn’t go away and the impact is still clear to see. Even if there is a golden bullet diagnostic test or therapy, the systemic health inequalities faced by the Rare Disease population will always prevent equitable and optimal access to these solutions. Patients can only access such technologies within the healthcare system that they live in, with the workforce that is available to them. A workforce that is currently not ‘rare aware’, having not had the appropriate foundational education in what rare disease is, its common challenges and the unique approach required to provide excellent care.
This statement from the King’s Fund about the ethos of Core20PLUS5 sums up the current status quo for Rare Disease in the UK:
“[Starting always with single condition areas] risks reverting to highly medicalised and siloed single-disease and condition-focused models of inequalities only, failing to recognise the many millions for whom inequalities in health do not come through these five routes alone but from multiple long-term conditions and the complexities that underly them.”
Action 40: addressing health inequalities for rare diseases through Core20PLUS5
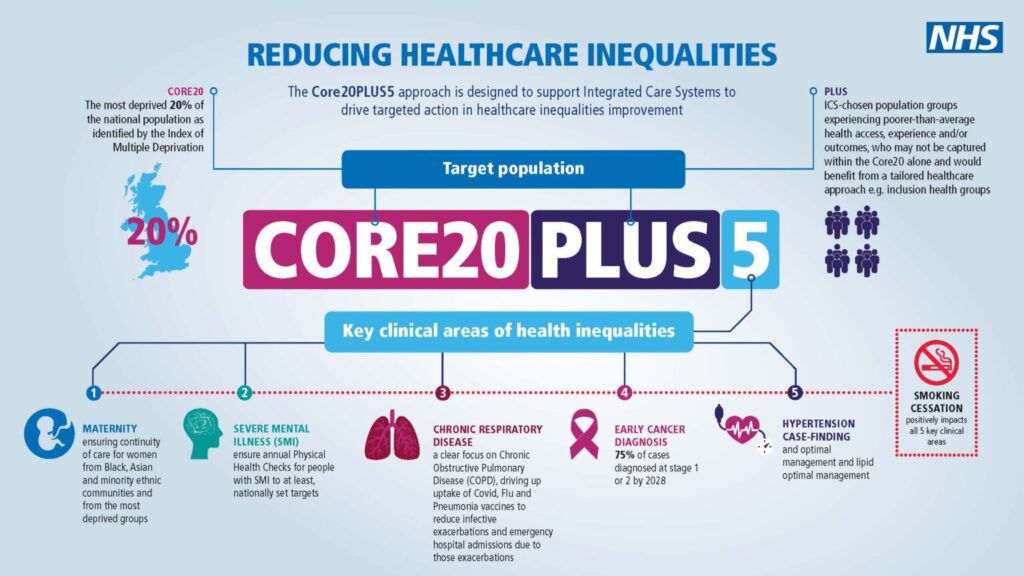
Core20PLUS5 is a national NHS England approach, to inform action to reduce healthcare inequalities at both national and system level. The approach defines a target population – the ‘Core20PLUS’ – and identifies ‘5’ focus clinical areas requiring accelerated improvement. It was launched for the adult population in 2021 and has since been adapted to create a similar framework for Children and Young People. In February the most recent update to England Rare Disease Action Plan included a new action (number 40) that caught my attention…
The Department of Health and Social Care recognised “that people with rare diseases experience inequalities in access to healthcare services and should be included under the NHS England Core20PLUS5 framework. Over the next year, we will develop an implementation plan for embedding rare diseases in the Core20PLUS5 framework with delivery of the plan over 3 years, from 2026 to 2028.”
The UK needs to keep up with the international community
This is the direction I want to see UK policy going, one where rare disease is a cross policy issue, reflecting the broad impact it has on the lives of people living with rare disease and their communities. Policies that protect and promote the rights of people living with rare disease need embedding at a Government level but also in individual organisations that provide or govern healthcare, employment, education, justice, etc. I am excited because this is, for me, a step in the right direction for truly improving the lives of the rare community. This could drive major improvements in awareness and create some framework for accountability. It also comes at a good time given the World Health Organisation’s plans to publish a Global Rare Disease Action Plan in 2027 (which the Lancet Commission will feed into).
Policy and public bodies need to lead by example to reduce stigma
Finally, the United Nations Resolution on “Addressing the needs of persons living with rare disease and their families” from 2021 states:
“Persons living with a rare disease and their families can be at greater risk of being disproportionately affected by stigma, discrimination and social exclusion, and that one of the major barriers to improving the inclusion and participation of persons living with a rare disease and their families in society is the lack of knowledge and expertise in the field and a lack of awareness regarding the issue”
We must lift rare disease out of a niche corner of policy and healthcare in order to address stigmatisation and prevent discrimination. By using well known initiatives and frameworks, such as Core20PLUS5, there is real potential to raise awareness in our public bodies and systems at scale and in a timely fashion. This advancement has the potential to increase visibility and reduce stigmatisation for the entire rare community.


